|
Hypothesis Explaining Prempro WHI Breast Cancer Findings (Dr.Tim)
|
||||||
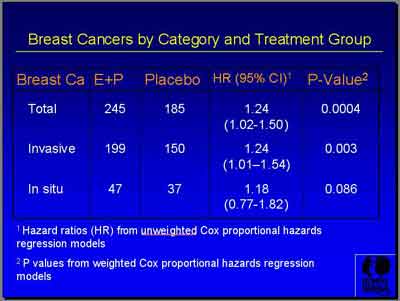
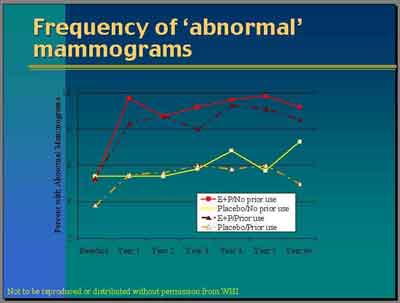
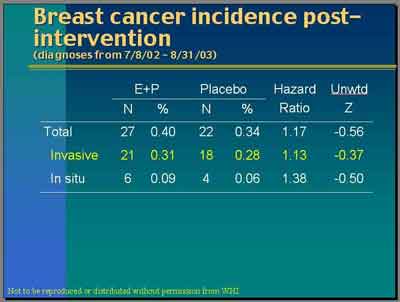
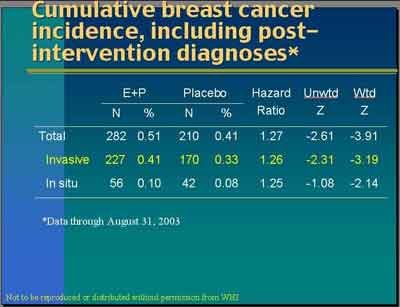
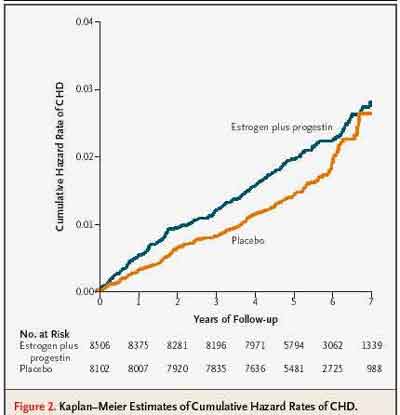
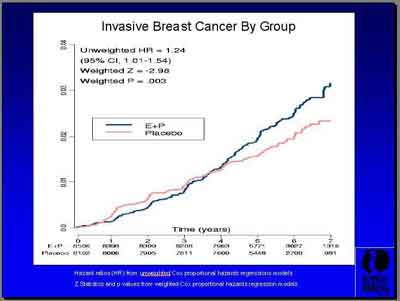
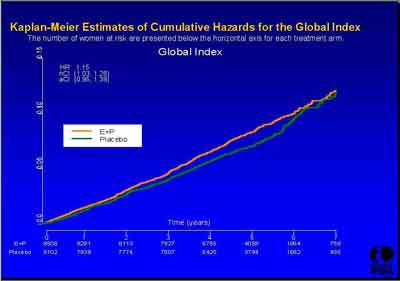
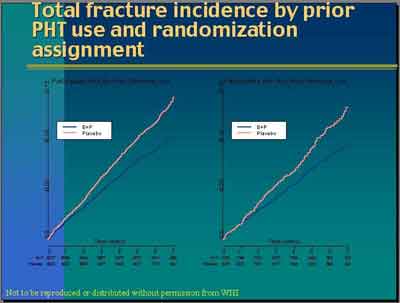
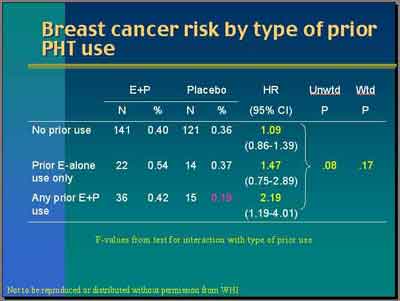
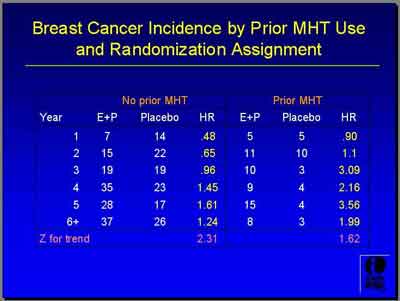
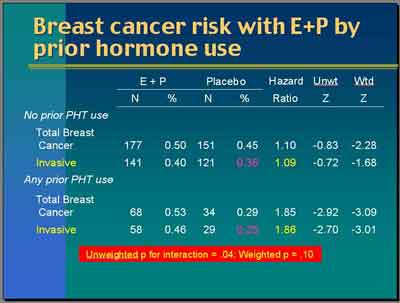
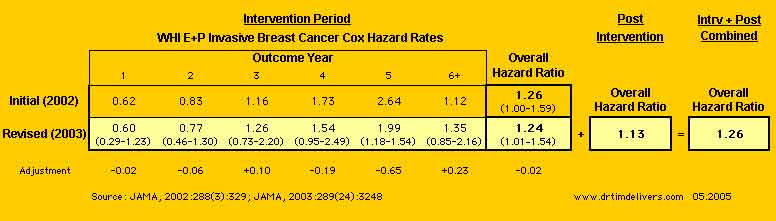
Breast cancer findings from the WHI are consistent with the hypothesis that: 1) Study patients with previous estrogen exposure have a number of larger undetected tumors, which are detected sooner after given Estrogen+Progestin compared to Placebo (Detectable tumors would have been already detected). This would especially be true for prior E+P exposure. 2) Study patients with no previous estrogen exposure would have a (possibly same or greater) number of smaller previously undetected tumors at baseline, which would take longer to detect after given Estrogen+Progestin compared to previous estrogen exposure (more undetected tumors). 3) Study patients given placebo would have minimal change in their tumor size during the study, with a lower detection rate during the study (the average age of patients was 63 and thus undetected breast cancers would be slower growing ones). 4) Study Patients given estrogen only also would have more but still minimal change in the size of their tumors and also with a lower detection rate, since estrogen stimulates tumor growth less than estrogen-progestin. 5) Giving estrogen-progestin (or estrogen) decreases new tumor formation and suppresses grade and nodal spread, but stimulates growth in size for existing tumors, increasing initial detection (would initially see fewer in-situ tumors compared to invasive). 6) A large number of Placebo patients who become non-compliant by starting E+P off-study, would increase the censored-after-6-months hazard ratio for breast cancer when they are excluded. This would lower the adherent Placebo rate and increase the adherent hazard ratio under intention-to-treat analysis, as reported in the study (if starting E+P increases initial detection, excluding those patients would fail to count cancers that would eventually be found anyway in the placebo group). 7) Earlier breast cancers detected would be more invasive (bigger tumors), later breast cancers more in-situ (finally big enough to detect but more benign). 8) Randomized studies of breast cancer survivors given hormones show lower mortality rates, consistent with this hypothesis. |
||||||
|
www.DrTimDelivers.com 05.14.2005
|
||||||
|
This review is dedicated with admiration to Donald Thursh, MD and
Mel Schoenberg, MD, who had it right from the very beginning. |
|